
My cardiologist never smiles, but I still love him
I’ve come to adore my cardiologist, even though he sometimes delivers disturbing news and forces me to contemplate my mortality every time I’m in his office. I didn’t always feel this way about him.
I first met Dr. B. Schwarz a year ago. I’d just had two mini-strokes and he came across as aloof, almost uncaring. (He never offered his first name and I didn’t ask.) The strokes had come as a surprise, presenting as left-side weakness and landing me in the Guelph ER on two successive days, just two weeks before my 60th birthday.
Both times, the symptoms passed quickly (in 15–30 minutes), but emotionally and psychologically, I was shaken. I spent a night in the hospital after the second one, the first time I’d done that since I was a teenager recovering from an appendectomy. And I couldn’t face going out in public for a week.
The mini-strokes were a rude introduction to my 60s, and also a reminder of my genetics. I’d witnessed both my parents having mini-strokes as they aged, about 20–30 years ago. “I guess it’s impossible to outrun your family history,” I wrote to close friends and family.
Dr. Schwarz was one of several specialists assigned to my case, to find out what caused my mini-strokes, or TIAs — transitory ischemic attacks — the two terms seem to get used interchangeably. More importantly, my cardiologist wanted to make sure it didn’t happen again. (A stroke is caused by a blockage in a blood vessel feeding part of the brain, either by a blood clot or by bleeding; in my case, it was the former.)
• • • • •
My first meeting with Dr. Schwarz was in his office. He was punctual and focussed, but far from warm. He was older than me (I judged), with a neatly trimmed beard, bushy eyebrows, thinning red hair and rimless glasses. He was short and slightly built, with polished shoes, baggy pants, and wearing a white lab coat with a stethoscope around his neck. He looked every inch an old school doctor.
And I don’t like to generalize, but his demeanour fit the East-European stereotype: polite but humourless, very clinical and scientific. A keen mind, devoid of emotion. He never smiled or laughed.
He began by asking me dozens of questions, like, “How much do you drink?”
I answer, “About seven drinks per week.”
“Is that one drink per day, or seven drinks on Saturday?”
It was hard not to chuckle at the way he was applying scientific inquiry to a personal question.
Then he sat me on an inclined table in his office and gave me a thorough physical exam. He listened very carefully to my heart, touching my chest and back intently with his stethoscope.
As he felt my pulse with his fingers I could sense his mind at work, absorbing all the subtleties of that simple, sensory, diagnostic technique. His touch was gentle and caring, and it showed an empathy that was at odds with his otherwise distant presence.
I was impressed. Then he quizzed me on my family history.
“My father had a major stroke at 64, and a series of minor strokes about 15 years later,” I summarized. “That’s what killed him, when he lost his ability to swallow.” Dr. Schwarz raised an eyebrow as he wrote on the notepad on his desk.
“Oh,” I added, “and he had atrial fibrillation.” Another raised eyebrow, more scribbling.
Despite being an in-demand specialist (one of three cardiologists in Guelph), Dr. Schwarz seemed in no hurry with me. His explanations were complex, he was prepared to go into detail, to draw a simple, child-like diagram of the heart on his pad of paper, and to answer all my questions. He didn’t condescend. If I didn’t understand anything, I could interrupt him, and his answers were thorough.
• • • • •
It had already been determined in the hospital ER that the cause of my strokes was not atherosclerosis, a buildup of plaque in my arteries from high cholesterol. So Dr. Schwarz wanted to look deeper into my heart function, to find out what had caused the little clots.
He immediately ordered two tests: a heart monitor that I would wear constantly for two weeks (taking it off only to shower), and an echocardiogram of my heart (an ultrasound, similar to the ones used to image babies in the womb), to see how it was working in real-time.
The results of these tests came promptly, within a week or two: I was told by phone that one of the tests was normal, but the other was not. Could I come in and discuss the results with Dr. Schwarz?
This time, I wasn’t surprised by Dr. Schwarz’s reserved composure when he entered the office. He seemed to relish explaining the results of the tests in detail. He showed me the pages of print-outs from the heart monitor. “Absolutely normal, no sign of atrial fibrillation, nothing to worry about.”
This was critical, and was the main reason for the uncomfortable, two-week test. As Dr. Schwarz explained, atrial fibrillation — a quivering, irregular heartbeat — is the cause of about a third of all strokes because it can cause clotting.
“It doesn’t mean you’ve never had an atrial fibrillation event, nor that you won’t go on to develop it,” he said. “It just means, we couldn’t detect it in this two-week window, and you don’t have it now.”
So, what was the “bad” news, from the 20-minute ultrasound of my heart, which was done in Dr. Schwarz’s office by one of his technicians?
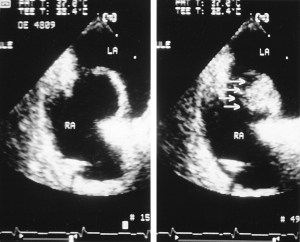
“You have an atrial septal aneurysm,” he said, (something I’d already been told over the phone), which also goes by its acronym, ASA. “It’s a bulge in the wall that separates the left and right atria of your heart, the two upper chambers. In your case, it bulges from the right side to the left, with every beat.” He drew a picture of it for me. (The ultrasound picture on top of this post shows an ASA, not mine, but similar — the labels RA and LA refer to the two atria, with the bulge in between.)
“Although it’s a rare condition, it’s not life-threatening, and you’ve probably had it all your life,” he explained. “But it has been shown to correlate with unexplained strokes, in younger people who don’t have other obvious risk factors like smoking, high blood pressure, athereosclerosis or obesity.”
Then I asked the question I’d been trying to figure out ever since the phone call from my family doctor a week earlier, which sent me scurrying to the internet to learn about my newly diagnosed condition.
“How does the ASA cause blood clots?”
Now Dr. Schwarz was in his element, explaining the chemistry of blood, the venous system (carrying blood to the right side of my heart) and the arterial system (the left side of the heart and the brain). If a stroke is caused by a “clot”, I imagined it being quite thick, but Dr. Schwarz used the term “thrombosis”, which he described as thickened blood. It could block a small artery in the brain, but then dissolve again quickly (the “transitory” part of the term TIA).
Strangely, the irregularity deep inside my heart could be a nexus for these jellylike clots, helping them form, and then launching them into my blood stream. This was all conjecture, because no test had spotted it happening, and there are other possible causes of stroke.
The only evidence Dr. Schwarz had was the CT scan (computerized tomography) that was done during my second trip to the ER. It showed a small spec of dead tissue in the right hemisphere of my brain, the smoking gun of a mini-stroke. The link to the ASA was hypothetical, but confirmed by medical studies, especially in the last 20 years.
• • • • •
Despite this startling revelation about my heart — the part of my body I thought had been performing so well as I ran 18 marathons over the last 18 years — I was actually relieved to hear about this new finding.
Now I had a “why” for my TIAs and the treatment wasn’t surgery, an implant, or even any hardcore drugs. The term “aneurysm” was scary, because a bulging blood vessel in the brain goes by the same name, and can also cause a stroke if it bursts. But my heart aneurysm was unrelated to that — the term simply meant an unusual protrusion inside my heart, something far less problematic, except for its association with blood clots. The condition occurs in about one per cent of the population and usually goes undiagnosed, with no symptoms.
My recovery from the two mini-strokes was nearly perfect — the slurred speech, left hand weakness and balance problems disappeared quickly, in both cases before I even got to the ER. I was lucky; the strokes were truly “mini”. The only vestige of those two events is droopiness in my left eye when I’m reading before bed — perhaps that’s the spot they saw on the CT scan, a minuscule loss of brain function.
TIAs aren’t crippling, but they’re serious for another reason — they are a warning of future, possibly disabling strokes. They suggest that bigger problems may be on the horizon.
My main treatment was started when I first went to the hospital, a daily blue pill that everyone calls a “baby aspirin” (even though we don’t give aspirin to babies anymore). Its function is to make my blood platelets less sticky, to reduce the risk of a small clot forming anywhere in my body.
Aspirin is informally called a blood thinner, but anti-platelet meds work differently than true anti-coagulants (like warfarin) and they are the first and least disruptive way to lessen the risk of a stroke — they only change the blood chemistry a little, by a “baby” amount.
There was symmetry in this: both my condition (atrial septal aneurysm) and my medication (acetylsalicylic acid) go by the same acronym: ASA. It was all very neat and tidy. I was reassured by the finding.
I was also prescribed two other medications: a blood pressure lowering pill (Ramipril) and a cholesterol lowering drug (Crestor), from the statin class of meds. Neither my blood pressure nor my cholesterol were considered “high”. My doctor has monitored them both for decades due to my family history; my running has been a non-medicinal way of improving my cholesterol profile. But with the evidence of TIAs, Dr. Schwarz wanted the readings down to half the normal threshold for both conditions, something that could only be done with medication he said.
Taking daily medication was new to me. And it was the most depressing aspect of my treatment. I hate going to the pharmacy and then transferring the pills to a weekly dispenser. In all cases, they give me no side-effects and are low-dosage, long-established drugs. For stroke prevention, the effectiveness of this three-med cocktail is well-proven.
I probably shouldn’t be complaining, but it felt like a threshold had been crossed, one I hadn’t considered before. Take these meds for the rest of your life, because this is the condition that could get you.
I raised the issue of the statin med with my family doctor. “Do I really need to be on that?” I protested, pointing to my high-normal cholesterol numbers from a recent blood test. I knew what Schwarz would advise but was hoping for a sympathetic ear from my progressive family physician, who was the ultimate arbiter of my treatment plan.
“Definitely,” was her reply, outlining the other benefits of statin medication, beyond lowering cholesterol. “It improves the health of your veins and reduces the risk of clots forming,” she argued, persuasively.
Dr. Schwarz had also raised another possibility, of a hole in the septal wall between the two upper chambers of my heart, the one that was bulging. He didn’t see it on the echocardiogram, but that didn’t rule it out, he said.
“We could do another test for this condition, called a patent foramen ovale (PFO), with a better-quality image, also an echocardiogram, but using a camera on a tube that we put down your throat to get it right next to the heart. We would do this under sedation, in the hospital.”
I’d had enough information for one day, and didn’t like the sound of this new test, the TEE (transesophageal echocardiogram), especially if it wasn’t likely to change my treatment — for information purposes only.
• • • • •
Months went by, I had no further mini-strokes, and I got used to taking my pills, a 10-second routine before bed. Things could be so much worse. My best friend died of lymphoma three years ago (in his late 50s); my younger sister is a breast cancer survivor; my cousin’s husband was diagnosed with ALS around the same time as my strokes. Was my little problem really anything to complain about? I am still able to run several times per week, and even train at a high intensity on the track with my running club, and race a few times per year — none of this activity is hampered by my heart glitch.
So, if the medications work without side effects, why question the treatment or fear the future? Get on with life was the advice of my family doctor, and she approved when I decided to stop working on Fridays, not to shed stress but to do other things with my time, to acknowledge what was now obvious: life doesn’t last forever!
But I began to get curious about the possibility of a PFO, a further defect in my upper heart. If I had even a remote chance of that, shouldn’t I know about it? It’s a relatively common condition (perhaps one in four people have it — astounding!), but mostly goes undiagnosed for a lack of symptoms. A PFO is the body’s failure to close the natural hole that exists in all human fetuses, the one that allows blood to flow between the two atria, bypassing the lungs before a baby is born.
This little circulatory short-cut usually closes at birth (or soon after) but sometimes the process is incomplete, allowing oxygen-poor blood to travel from the right atria to the left atria, which is supposed to carry only oxygen-rich blood. A PFO can allow clots to travel from the venous side of the circulatory system (where they are more common) to the arterial side (where they are more threatening) without being filtered through the lungs first.
Dr. Schwarz doubted that this was happening in my case, because he’d seen no sign of it on his echocardiogram (no “inter-atrial communication” he wrote in his report). “But it’s not proven that you don’t have it,” he observed, “we can only do that with a TEE.” If they did find a PFO, then they’d consider the option of closing it, with a patch installed via a simple catheter procedure.
The clincher for me was discovering on my own that 7 out of 10 cases of atrial septal aneurysm also involve a PFO. WTF? Why hadn’t Dr. Schwarz told me that?
At my next regular visit, I told him about my change of heart. “I’d like to have the TEE,” I said.
He agreed immediately, then explained the test, and said he’d performed them routinely when he was a resident in Kitchener, which is where my test would take place. The TEE carried little risk, he said, although I would have to sign a waiver in case the tube damaged my throat or vocal chords (gulp).
• • • • •
The TEE involved half a day in the hospital, with the actual procedure taking about 30 minutes. I was sedated intravenously, so I remembered nothing after rolling over to face the cardiologist who did the intubation.
Before going under, he advised me, “you likely have a PFO, don’t be surprised.”
But he changed his tune when I woke up, informing me — while I was still too groggy to take it in — that my heart was “great, absolutely normal.” In fact, he didn’t even see evidence of the aneurysm that had been diagnosed by Dr. Schwarz.
Later that evening, the news sank in, and left me a little depressed. The ASA, my ASA, didn’t exist after all. Good news, right? That’s what all my friends thought, at least the ones I’d told about the test. No, not good news, at least not from my perspective. If the ASA hadn’t caused my strokes, then what had? I was hanging my hat on that simple explanation, and now it had suddenly vanished.
Were my strokes “cryptogenic” after all, uncategorizable, with all the attendant doubts and unknowns? Did I have atrial fibrillation occasionally? Is that what made me anxious at unexpected times over the past three years, as if my body was about to fail in some catastrophic way? Or was that just fear of fear itself, from seeing what my parents suffered, a mental health issue that should be treated with Cognitive Behaviour Therapy, as my family doctor suggested?
• • • • •
As always, Dr. Schwarz was calm and cool when I saw him last week. He had the TEE report open in front of him and seemed unsurprised at the result. As he examined me with his stethoscope — always wanting to listen in case he hears something new or significant in my chest, or maybe it’s just his habit, something he does with every one of his patients — I was peppering him with questions. And he was answering, even as he listened to my heartbeat, multi-tasking.
“No PFO,” he says.
“Doesn’t that contradict your earlier findings?”
“No,” he answers, “no contradiction.”
“But the Kitchener cardiologist said there was no ASA,” I interrupt. “Was your test a false positive?”
Dr. Schwarz takes the stethoscope out of his ears and consults the hospital report. “Maybe I missed something,” he stammers. It’s the first time I’ve seen a crack in his professional cool, even a fraction. Does he doubt something?
“Wait a minute, I’m going to check the echocardiogram results,” he says, leaving the room.
He’s back very quickly and beckons me through the open door. “Come and look.”
He leads me to darkened room with a computer and monitor. He offers me a rolling chair with no arms, beside his. Then he plays a short video, my echocardiogram from nine months ago. It’s a startling image, on a dark background with the outlines of the heart chambers in light colour, and everything in fast, jerky motion, like an animated GIF online, with whorls of colour that show blood flow.
“Here,” he points to the bottom of the screen. It takes some imagination, because the image is rotated 90 degrees, with the right side of my heart at the bottom. But then I see what he’s referring to, a sudden bulge with every heartbeat, where the straight septal wall stretches briefly sideways, into the left atrium, then returns to normal.
It’s hard to judge the size of the images because the whole video is enlarged, well beyond the size of a human heart, which is like a fist. It is alarming to watch, a weird, pulsating deformity. But Dr. Schwarz immediately reassures me.
“It’s not a remarkable ASA,” he says, “but it is unmistakeable.” (His language is always this precise.) He seems satisfied as he reviews the findings he wrote in his report on the test: “Aneurysm of the atrial septum with bulging towards the left atrium … could be a nidus for platelet aggregation and micro emboli” — in other words, the clots that caused my mini-strokes.
Then he adds, “I stand by my diagnosis.”
Having seen it with my own eyes, I tend to agree. I’d watched several similar videos of ASAs online, and mine resembles those. Back in his office, I ask why the second imaging technique delivered a contradictory conclusion to the first.
He explains: “The transthoracic echocardiogram is actually better for imaging the ASA, while the transesophageal echocardiogram is better for diagnosing a PFO.” (That’s the level of medical jargon you have to learn in order to understand a cardiologist!)
Dr. Schwarz concludes: “You have an ASA, but not a PFO.”
He goes on to talk about atrial fibrillation again, something he’s still wary of in my case, almost as if he expects it to crop up. “It occurs in about 10 per cent of people by the time they’re 80,” he says, “but you’re young, not something to worry about now.”
I’m overcome with emotion with all this news, and especially from watching the video. My eyes are watering and I’m lost in my own thoughts, but Dr. Schwarz doesn’t notice, or doesn’t let on that he notices.
For once, I’m speechless, with no more questions. He folds his arms and looks at me carefully. There’s no pat on the shoulder, but he says, “We’re doing the right thing in your case. I’ll continue to watch you carefully.”
He’s saying, I’ve got my eye on you, I’m training all the wisdom and experience of a career cardiologist on your case, which isn’t all that complicated or special. I’ve seen this before, and you’re going to be okay.
Finally, he asks, “Any more questions?” He won’t leave before my curiosity is sated. He’s spent nearly 30 minutes with me today because of my myriad queries.
“No,” I answer. “Thanks very much.”
He quietly closes my file and says, “I’ll see you again in six months,” then gets up and walks out of the office, leaving the door ajar.
I’m deeply grateful for his focussed and professional attention. He would never be a friend, but in every other way he exercises the deepest possible care for his patient.



What a story. I am so glad it has a happy-ish ending. And I’m reminded of what a great thing we have in medicare. Look after yourself and keep your friends and loved ones close, JIC.
Wow, Art. Thanks for sharing a very personal medical situation…your self-advocacy and research is impressive. Glad to hear your health is under Dr. Schwarz’s watchful eye!
Great explanation of the medical system and your experience. You have a very enquiring mind as well as a gift for interpretation and documentation.
Art, you are such a wonderful writer. I can’t begin to remember all the medical terms but your portrait of Dr. Schwartz is so strong. And you achieve your own story through telling us about him. Fantastic and fascinating. xo
I think I might have told you this story Art, but my Mom has had some heart irregularities and has had to see a cardiologist in her town. No serious concerns, but the contrast in medical styles is significant. At one appointment she went in after waiting to see the Dr. for some time, he does not even look up, he looks down, scribbles, and says “August.” My mom says “August?!?” He says, “I will see you again in August. Tests were good, nothing to worry about.” I am paraphrasing liberally here, but the main point is that he was so dismissive and so gruff and so unlike your Dr. Schwarz. I am blown away by your attention to the details… right down to the baggy pants and the raised eyebrows. Beautiful story. xoxo
Ugh. That’s terrible David. Although the system can be good, it’s also luck of the draw as well, I guess! Thanks for your comment.